
Big Pharma has stepped up its lobbying game ever since the federal NDP struck a deal to prop up the Liberals’ minority government contingent on several big-ticket items — including progress on national pharmacare.
Announced last March, the Liberal-NDP agreement hinges on the federal government launching a dental care program for low-income Canadians and “continuing progress towards a universal national pharmacare program by passing a Canada Pharmacare Act by the end of 2023.”
From March 2022 to January 2023, large pharmaceutical companies and lobby groups recorded just over three times more lobbying communications with Health Canada than their yearly average from 2015 to 2019, according to data compiled by the Council of Canadians. The Council of Canadians also identified an uptick in the insurance industry’s lobbying of Health Canada between March and January — a fourfold increase compared to the 2015-2019 average.
Public statements from large industry groups, like Innovative Medicines Canada, welcome the federal government’s efforts to improve access to pharmaceutical drugs but insist a national program must build on the existing private system and improve access for uninsured and underinsured Canadians.
Similarly, a written statement from the Canadian Life and Health Insurance Association said it is “supportive of the goal of universal pharmacare” and it's crucial the new program focuses on Canadians without coverage and “does not erode the benefits over 27 million Canadians depend on.”
Many companies echo the association’s statement, including Hoffmann-La Roche. In an email, the company’s vice-president of strategic communications Laura Pagnotta added that “a public-private model in drug coverage should be maintained so all Canadians have the same, or better, coverage than they currently have today.”
This goes against advocates’ visions for a national public program that covers all Canadians. Pharmaceutical and insurance companies’ desire to maintain the current patchwork system and merely have the federal government “fill the gaps” left by private coverage protects the industry’s bottom line because a single-payer program would drive down drug prices, Donya Ziaee with the Council of Canadians wrote in a blog post last fall.
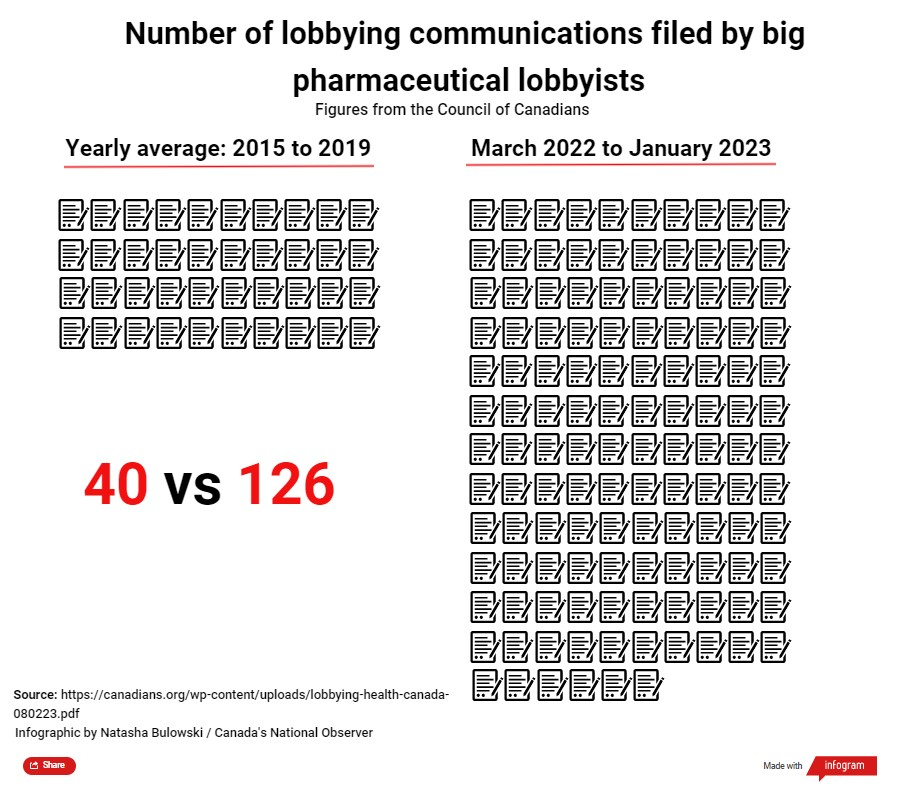
The lobbying numbers were revealed at the launch of the Fight for Pharmacare Alliance in Ottawa on Feb. 9. The national coalition includes the Canadian Labour Congress, the Canadian Health Coalition, Canadian Doctors for Medicare and Coalition solidarité santé.
Progress on implementing pharmacare has been “excruciatingly slow,” said Nikolas Barry-Shaw, a trade and privatization campaigner with the Council of Canadians. Lobbyists from the two industries that stand to lose the most from a public pharmacare plan — pharmaceutical companies and insurers — have lobbied the Health Ministry 150 times in nine months, he said at the press conference. According to Barry-Shaw, this corporate influence is the answer to why pharmacare is moving at such a slow pace, and the new alliance will fight to accelerate it.
In an emailed statement, Innovative Medicines Canada’s director of media relations Marise Varanda said the national association represents Canada’s innovative pharmaceutical industry and “actively meets with government stakeholders to discuss various topics of importance to the health of Canadians.”
“If a health-care system excludes just one Canadian to save a buck or to make a profit, that system is wrong,” patient advocate Bill Swan said at a news conference when the lobbying data was announced.
Swan has spent a majority of his 60 years pushing for national public pharmacare for all. Born in 1963 with severe asthma, Swan’s treatments and medications were covered for the first chapters of his life, thanks to insurance through his father, who was in the Armed Forces. But that all changed after Swan finished his undergraduate degree.
An insurance company turned him away because of his underlying condition: asthma.
“That led me to stop taking my drugs because the economy at that time was not the best,” Swan told Canada’s National Observer in a phone interview. “That summer, I ended up in the ER four times.”
These repeated hospitalizations prompted him to think about how much it costs the health-care system to deal with one of his asthma attacks.
“If I'd had my drugs in the first place, I wouldn't be here,” he said.

Repeated severe asthma attacks left Swan with scarred lungs and chronic obstructive pulmonary disease, he said.
The Liberal-NDP deal’s language on universal pharmacare is vague and doesn’t specify whether a national program would be publicly funded, the Council of Canadians has pointed out.
A public-private drug coverage system like Innovative Medicines Canada and the Canadian Life and Health Insurance Association describe is a flawed strategy, says Sharon Batt, a health policy expert and adjunct professor of bioethics at Dalhousie University. Instead of a patchwork of private coverage where the government picks up the tab for uninsured Canadians, she advocates for a single-layer public program for several reasons.
For the most part, under a public-private system, the healthier, wealthier people with good-paying jobs would keep private plans while drug coverage for the unemployed, elderly and those likelier to have chronic conditions requiring expensive and ongoing treatment would fall to the government, Batt said in an email to Canada’s National Observer.
She added that some drugs are now so expensive that private plans are starting to increase co-pays, introduce caps and cut some drugs from their lists, which can affect those who depend on their drug coverage.
Each year, Rowan Burdge pays roughly $10,000 out of pocket for life-sustaining medications and supplies. Burdge is a Type 1 diabetic.

“If I don't take my insulin, I will get very sick and have to go to the emergency department, and that causes just a lot more issues and a lot more cost down the road,” Burdge told Canada’s National Observer. “It's all about providing preventative care, providing people with basic human rights, which includes medications, and making it so that people aren't having to pay a lot of money out of pocket for things that they need just to survive.”
A 2018 report by the Canadian Federation of Nurses Unions found approximately one in five Canadians reported having no or inadequate coverage for their prescription costs. About half are without coverage because they don’t qualify for public drug coverage and don’t have private insurance, according to the report.
The federal government is taking “significant steps towards tabling a Canada Pharmacare Act in 2023,” according to an emailed statement from Health Minister Jean-Yves Duclos’ office.
Some of the steps taken towards national pharmacare included establishing a Canadian Drug Agency Transition Office to work with provinces and territories to develop a mandate for the Canadian Drug Agency in 2021, the email noted.
Natasha Bulowski / Local Journalism Initiative / Canada’s National Observer

- Natasha Bulowski
- Journalist
- @NBulowski
Keep reading




So now it looks as though we
So now it looks as though we have to put a limit switch lobbying? a maximum number of lobbying visits per topic to the Hof C, and Senate, and The Provincial Legislature(s).
Once again this shows that corporate Canada owns the Federal and Provincial government.
This is an excellent article
This is an excellent article anam opened my eyes on the need for a national pharma-care program. I enjoyed the article but I suggest you correct the prononciation of Dalhousie University. .
This terrible situation is
This terrible situation is made worse when realizing that the salaries and business expenses of the lobbyists are likely fully tax deductible corporate business expenses. The paradigm of modern medicine is to palliate with treatments that provide life-time annuities to shareholders. The profits from this industry pay for political parties, research and medical schools.
Excerpt:The Situation of Human Rights Defenders of Lyme and Relapsing Fever Borreliosis Patients: Edition One:
On October 24, 2017, the United Nations (UN) Special Rapporteur (SR) on the right to health, Dainius Pūras, presented his report on corruption to the UN General Assembly. He told his audience, “In many countries, health is among the most corrupt sectors; this has significant implications for equality and non-discrimination “... He noted some are related to the global pharmaceutical industry and others from “institutional corruption” and emphasized the “normalization” of corruption in healthcare which includes practices undermining
medical ethics, social justice, transparency and effective healthcare provision, as well as illegal acts. Many researchers and scholars support the SR’s findings and note how the corporatization of medical practice has contributed to this situation and the loss of medical professional autonomy.
Canada, along with other nations agreed to support the CDC and follow its lead. The CDC is a highly conflicted organization and in need of reform as is PHAC.
Thanks for this important
Thanks for this important article. Recently, federal health minister Jean-Yves Duclos appointed Thomas Digby, a pharmaceutical investor and legal advisor to the industry, to head up the Patented Medicines Prices Review Board. Digby’s work over the last 25 years has been to support Pharma’s efforts to make massive profits, especially by extending patent rights and ensuring countries uphold this awful international stranglehold on our ability to produce and access needed and affordable medicines. Digby, for example, urged Canada to oppose the TRIPS Waiver on the COVID vaccine because our #1 job is to defend and uphold patent rights, not access to the vaccine during this pandemic. So people like Rowan Burdge who now are struggling with an out-of-control pricing system for essential medicines like insulin likely will be in for an even more difficult future. Independent Voices for Safe & Effective Drugs has protested about this appointment. See https://www.ivsed.org/_files/ugd/966b2a_018ddde880e44c46a5b9a3305074329b...
We used to have a strong,
We used to have a strong, independent civil service advising ministers. This would seem to be another case of corporate capture. Geoffrey Chaucer 14th century author of the Canterbury tales wryly noted the physique and the pharmique travelling together, each living off the guile of the other. We are in danger of losing all our democratic institutions because of the increasing influence of industry lobbyists.
Government doesn't care
Government doesn't care enough about nutrition, vitamins, hormones and other naturally occurring substances that affect our health. Pharma doesn't care at all about anything that doesn't get it an income stream. Nobody gives a fig about side effects and adverse outcomes.
Comments